Rethinking Bone Graft:
Adapting to Nature Rather Than Fighting It
Alveolar bone resorption is an inevitable biological process, particularly within the first 6 months after extraction. In more than 80% of cases (Class I resorption), labial bone loss occurs, leaving only the palatal plate, which complicates implant placement. Even with bone grafting, resorption continues, leading to peri-implant bone loss and instability.

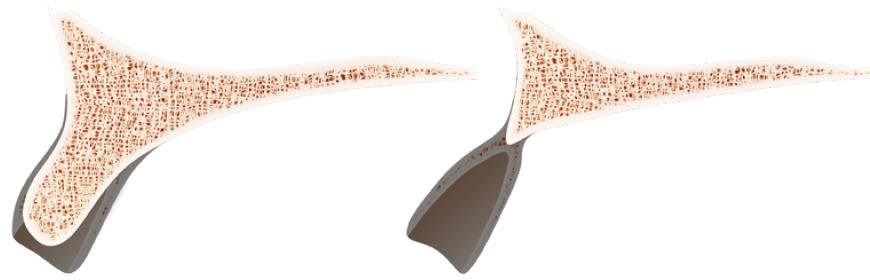
For years, implant dentistry has focused on preserving alveolar bone through methods such as immediate implant placement, GBR, and ridge augmentation. However, none of these approaches can fully prevent bone resorption. Even successful ridge augmentation often results in continuous bone loss after 10 years, leading to complications.
Wouldn’t focusing on implants designed to align with physiological processes, rather than opposing nature, lead to higher predictability and long-term success?
It’s better to utilize ‘Existing bone’ rather than ‘Regenerating lost alveolar bone’ for implant!
With this in mind, MegaGen has developed and adopted the use of basal bone, a stable human skeletal tissue that maintains its integrity over time, along with adaptive implant designs.

Redefining Anterior Atrophic Ridge Treatment:
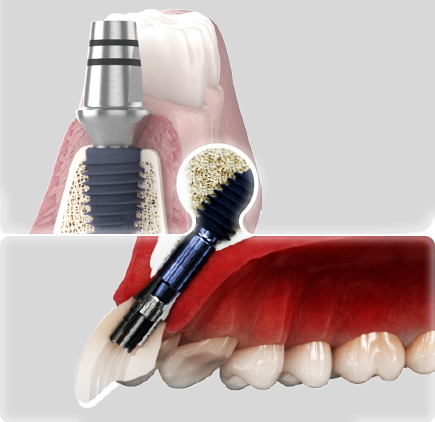
ARi
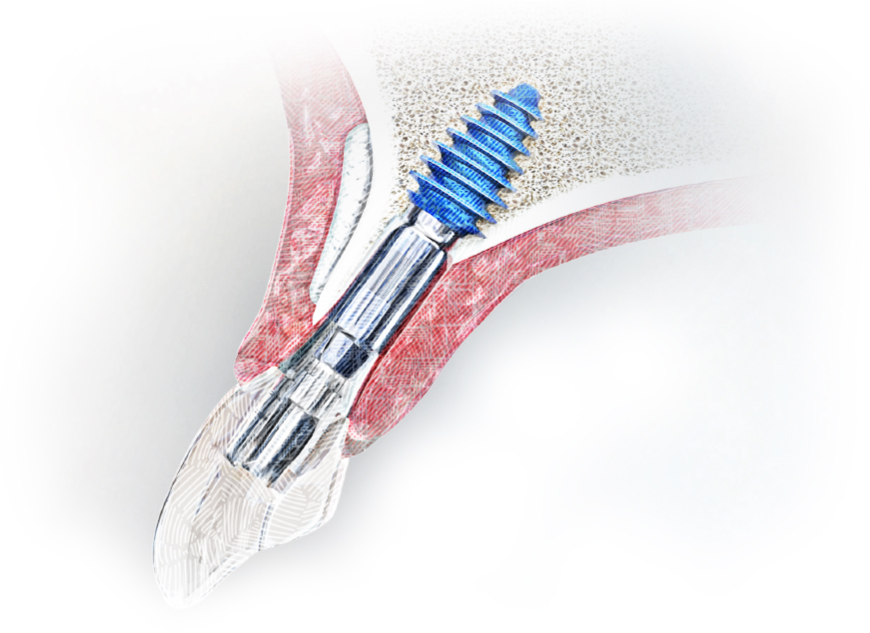
- · Acquires strong stability and osseointegration from unresorbed basal bone, not atrophied alveolar bone
- · Implant body design improves post-care effectiveness
- · Long-term stability is secured, even without the alveolar bone
01. Strong joint stability
10° external conical hex provides strong bonding with abutment
02. Soft tissue friendly design
Rapid regeneration of soft tissue by facilitating generation and proliferation of HGF*-cells and subsidence prevention function
03. Guaranteed strong initial stability from basal bone without bone volume restoration
Deep thread & KnifeThreadⓇ design for smooth implantation without bone destruction
04. Favorable surface for prevention and management of peri-implantitis
Minimizes adhesion of foreign substances around implants, and easy removal of foreign substances if it occurs
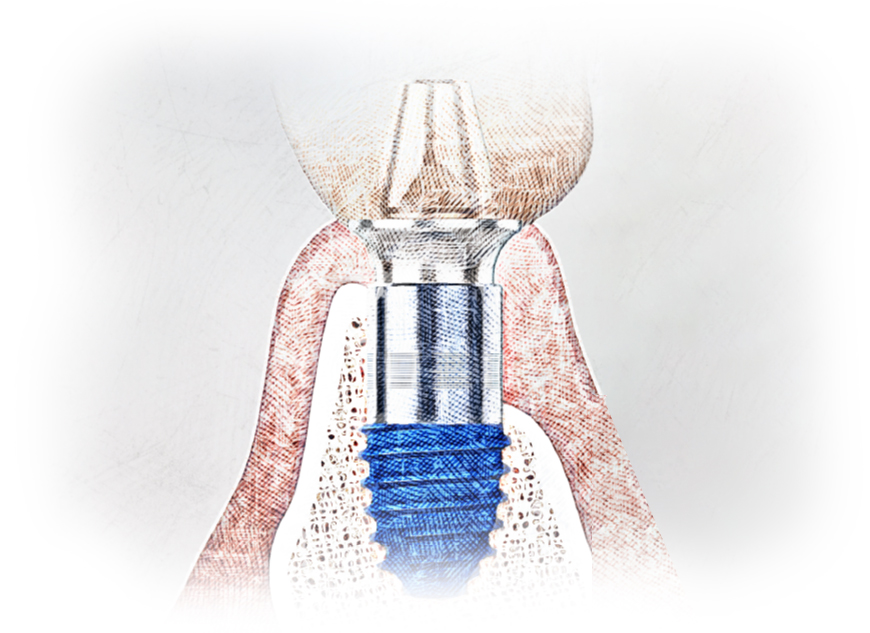
05.Strong osseointegration force in basal bone maintains stability even if alveolar bone is lost
Incorporating calcium ions that create bone on S-L-A surface increases rate of osseointegration by more than 15%. Blue surface color is evidence of calcium ions!
06.High strength guaranteed even in narrow zones
200% (2-fold) improvement in strength (compared to our implant system for the narrow zone), and straight body design without stress concentration
Clinical Case
ARi® enables implant placement in the desired location even in an extremely thin ridge anterior region without bone augmentation, and secures sufficient fixation and stability, so there is no concern about complication treatment.
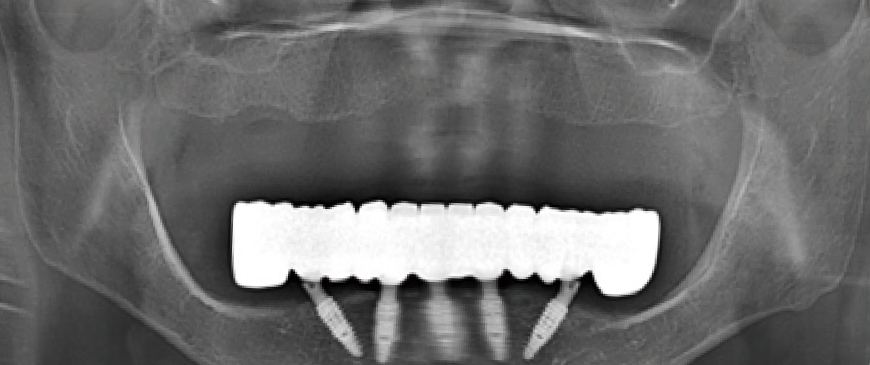
Fig 1
A female patient in her early seventies, physically healthy, experienced instability with her upper denture.
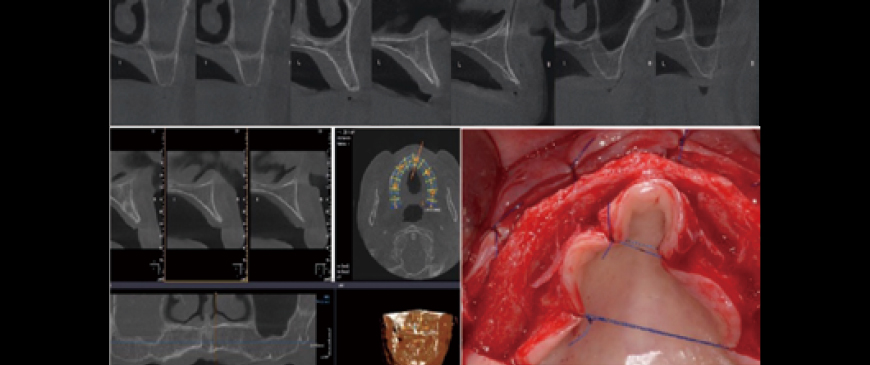
Fig 2
Pre-surgery CBCT state / Flap detached. The anterior region showed a very thin ridge. Could implants really be considered in such a ridge? This case required accepting ridge augmentation, which involved a long treatment time and a very high risk of complications.
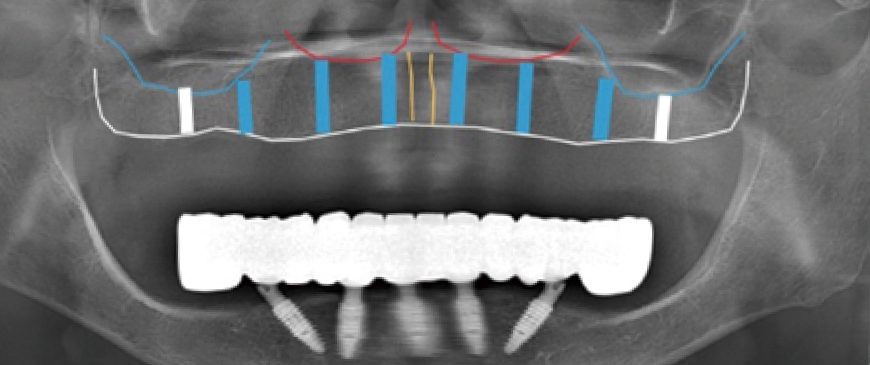
Fig 3
The plan involves placing 6 to 8 implants, evenly distributed across the available space.
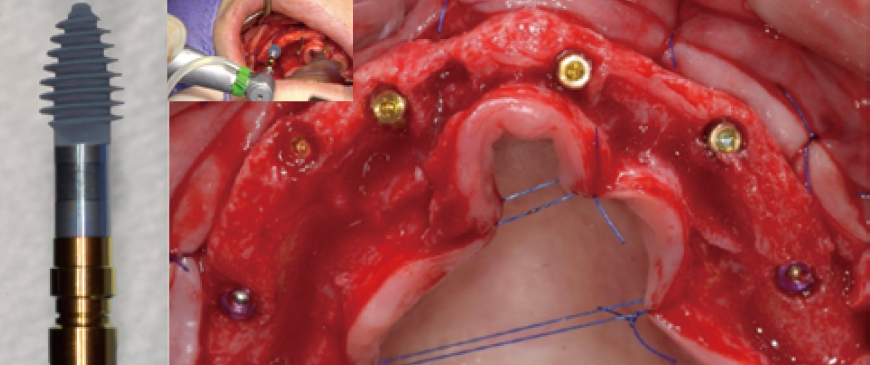
Fig 4
It is always better to choose ‘Palatal positioning’ in the Upper Thin Ridge for long-term stability. In this case, 4 ARi (3.2) 4.5x7.0(6) implants and 2 BlueDiamond implants were placed, totaling 6 implants in ideal positions. The Knife Thread of the ARi implant smoothly integrated into the thin ridge without causing any damage, ensuring optimal stability and positioning.
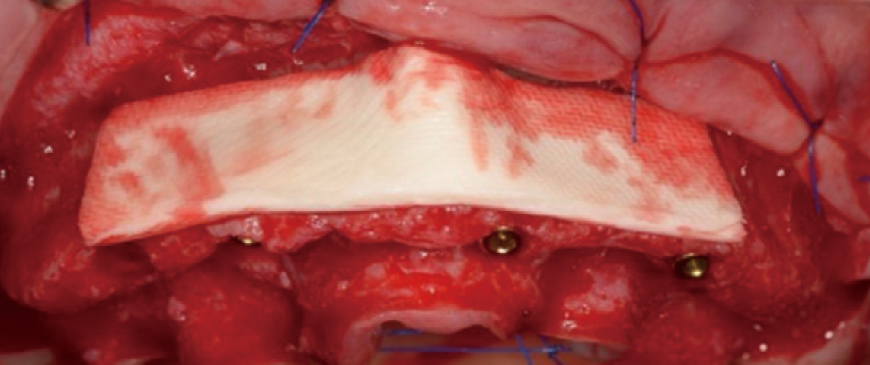
Fig 5
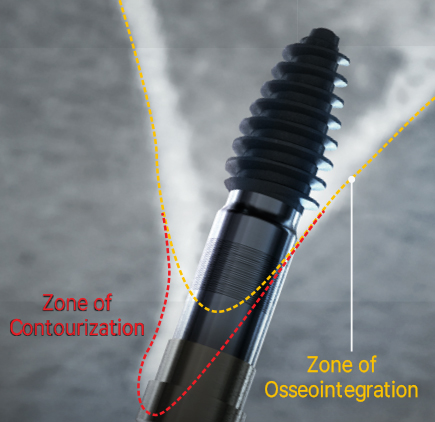
Ossix Volumax was used to create the contourization. This material ensures the desiredvolume and contour in the implant area. by performing the surgery in a simple manner, the chance of early complications caused by the surgery is almost eliminated.
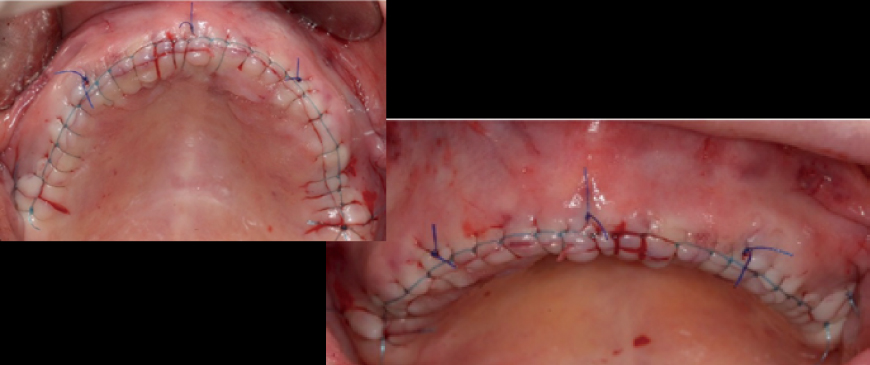
Fig 6
Since only minimal augmentation (contourization) was performed using Ossix Volumax, the suturing could be done easily and simply without the need for a separate periosteal releasing incision.
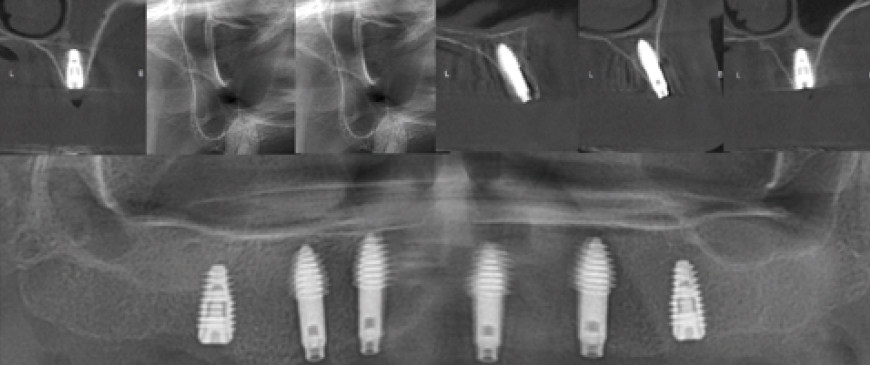
Fig 7
Post-surgery panoramic and CBCT radiographs show that all implants in the posterior and anterior regions were placed in stable positions. Since the fixture threads of all implants were securely integrated into the bone, a secondary surgery was scheduled approximately 10 weeks later.
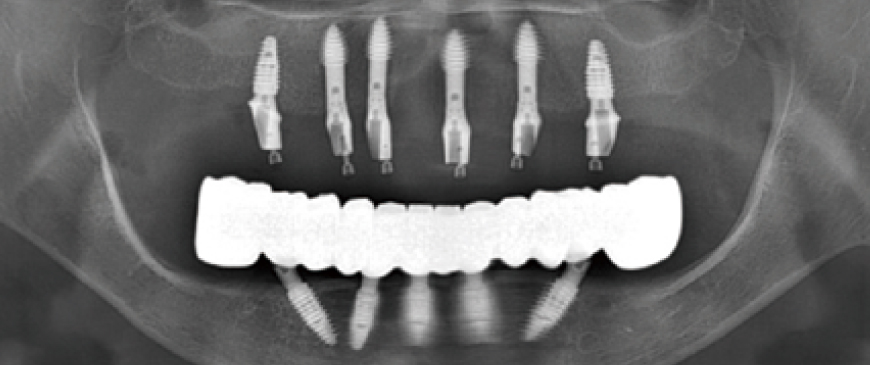
Fig 8
Custom abutments and PMMA temporary restorations were placed on the entire maxillary implants. The condition was stable both aesthetically and functionally.
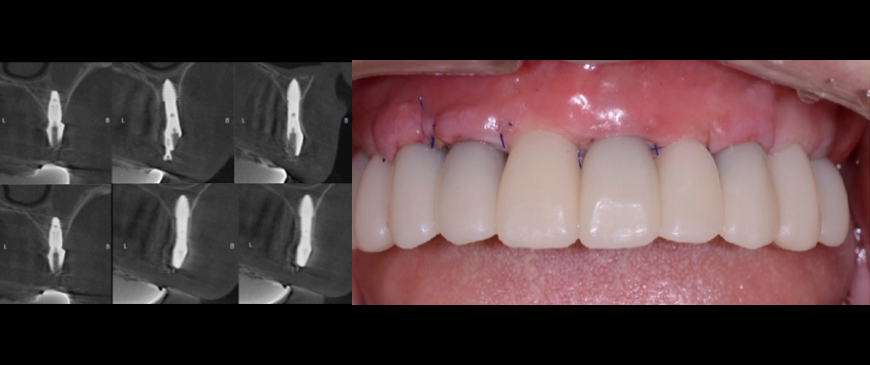
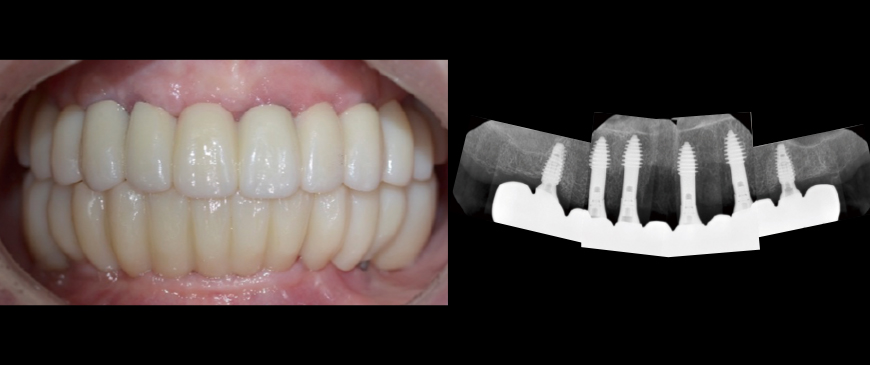
Fig 9
Approximately 6 months after the maxillary surgery, the final prostheses were placed on both the upper and lower implants. The FP1 (Functional Prosthesis 1) was successfully achieved on a thin ridge, utilizing a minimally invasive approach and a short treatment period. This was accomplished without sacrificing the integrity of the thin ridge or requiring heavy GBR.
ARi® in the Lower Anterior Extremely Thin Ridge in Full-Mouth Mandibular Implants.
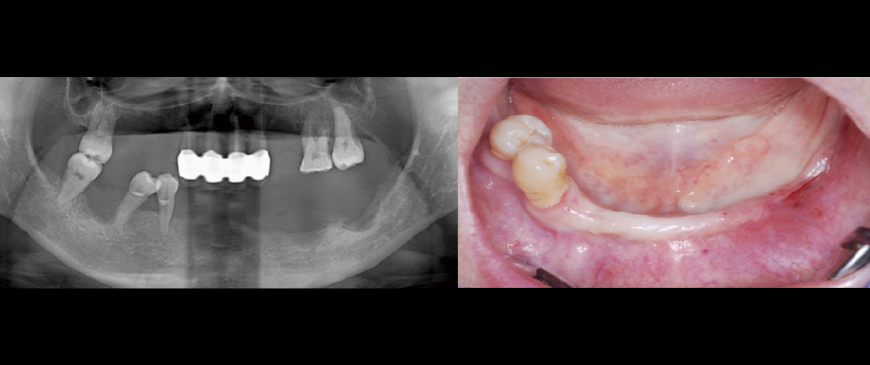
Fig 1
A woman in her late 40s presented with multiple tooth loss and chewing difficulties due to severe periodontal disease. The mandibular anterior region had a thin ridge, but vertical dimension was maintained in both jaws. The upper jaw was to be restored with a partial denture, while the lower jaw was treated with All-on-6 implants to address vertical dimension loss in the left posterior region.
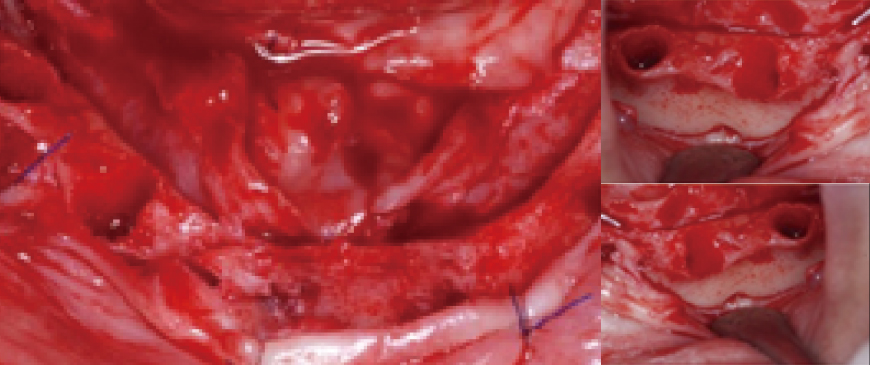
Fig 2
The 2 right premolars were extracted, and a flap raised. Identifying the mental foramen location is key for All-on-X, after which placing tilted implants at 30- 45° completes half the procedure.
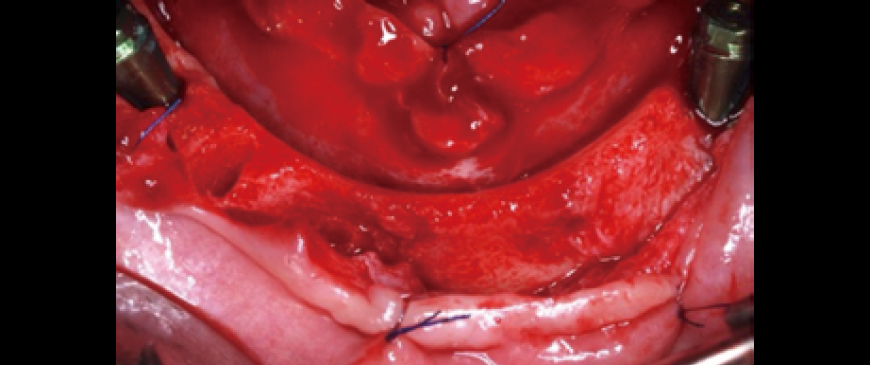
Fig 3
One tilted implant was placed on each side (left and right).
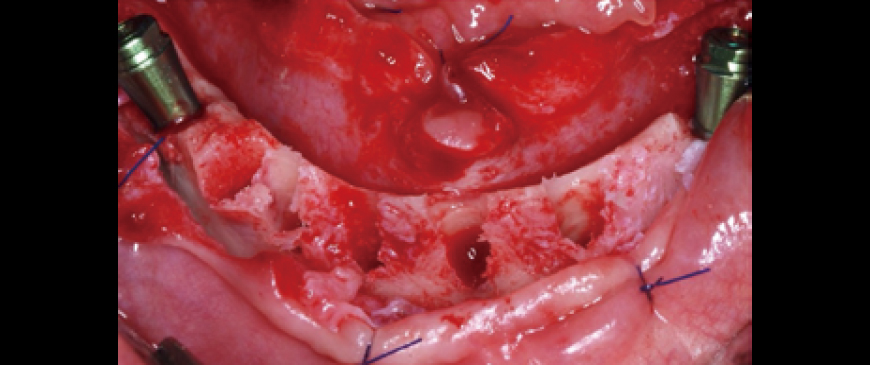
Fig 4
4 straight implants were placed between the two tilted implants. Due to the very thin alveolar ridge in the anterior area, a 3.5mm ARi fixture was chosen.
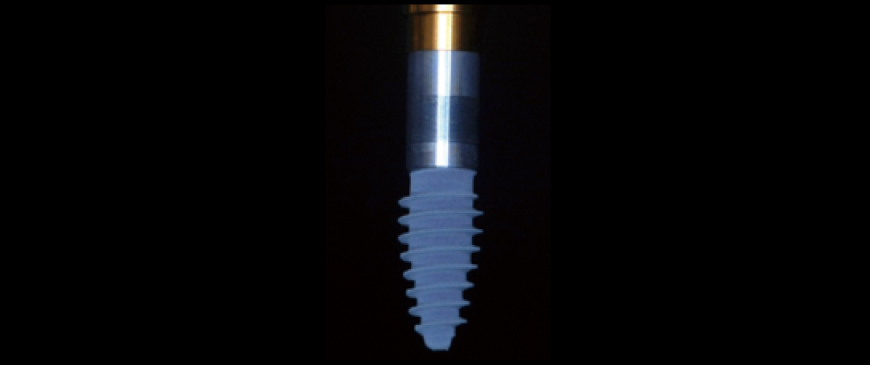
Fig 5
After drilling with a 3.3mm drill, the ARi fixture provided excellent initial stability. The bone density was D2, and an ARi (2.8) 3.5x9.0(6) fixture was placed to cover the labial defect.
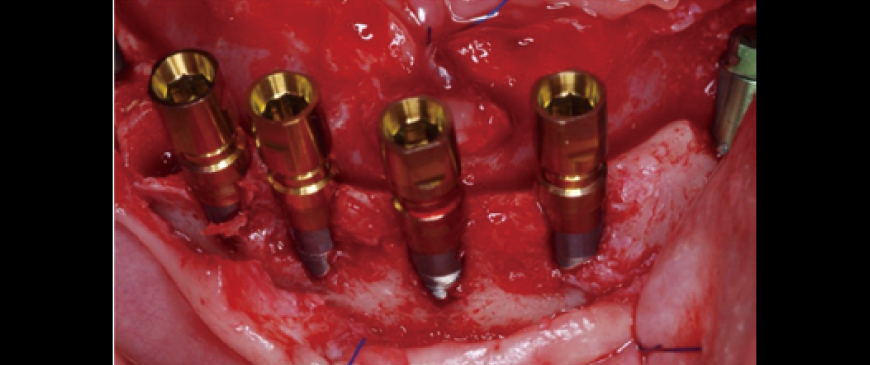
Fig 6
Four ARi implant fixtures were placed. A 5-6mm dehiscence occurred on the labial side, but it was limited to the machined cuff.
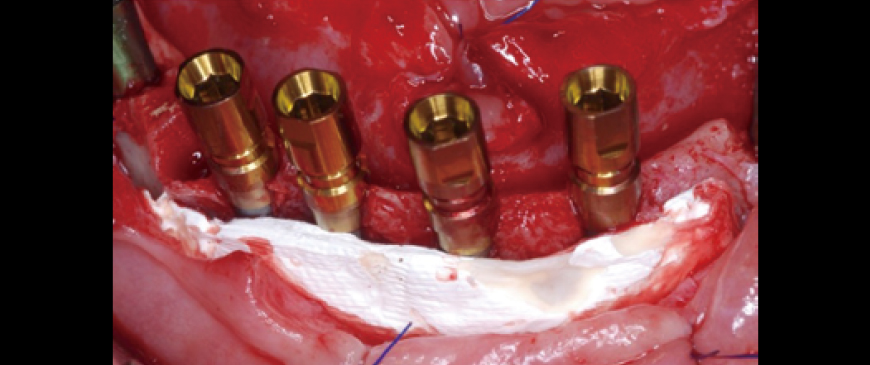
Fig 7
To prevent potential visibility through the thin biotype gingiva in the future, a layer of Ossix Volumax (10x40mm) was placed.
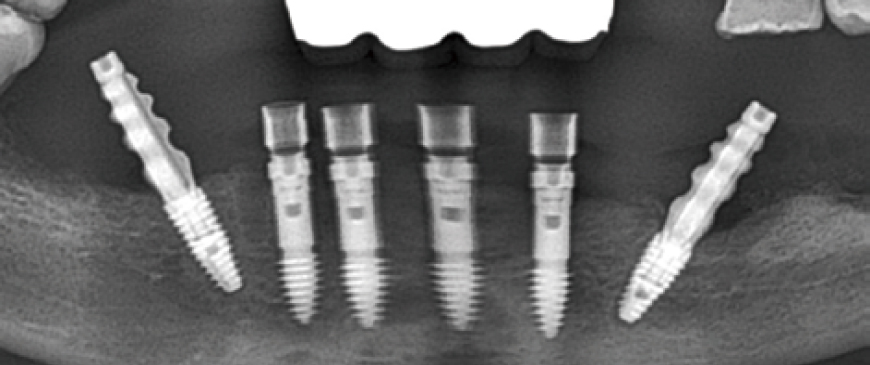
Fig 8
Post-surgery panoramic radiograph. Immediately after the surgery, impressions were taken to prepare provisional prostheses.
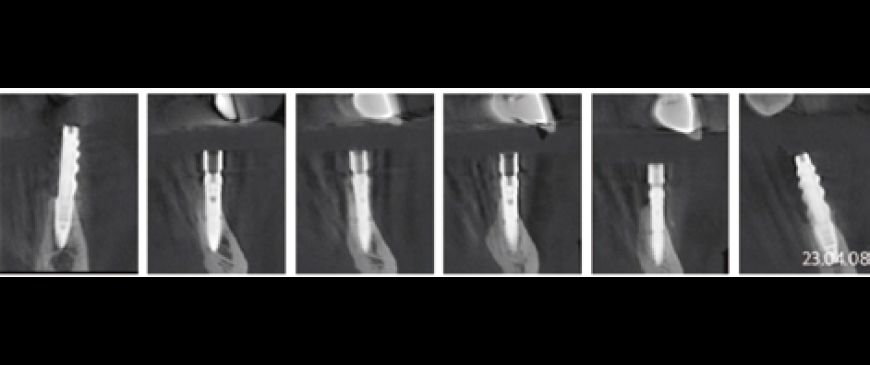
Fig 9
Post-surgery CBCT radiograph. All ARi implant threaded parts were properly positioned within the alveolar bone
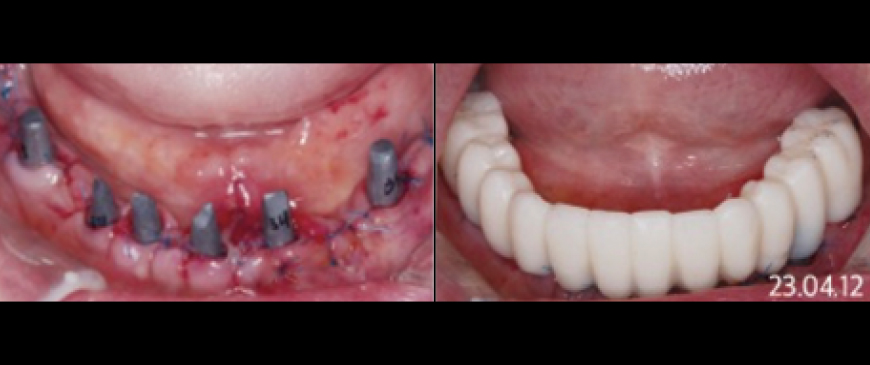
Fig 10
Four days after the surgery, custom abutments and a PMMA bridge were placed.
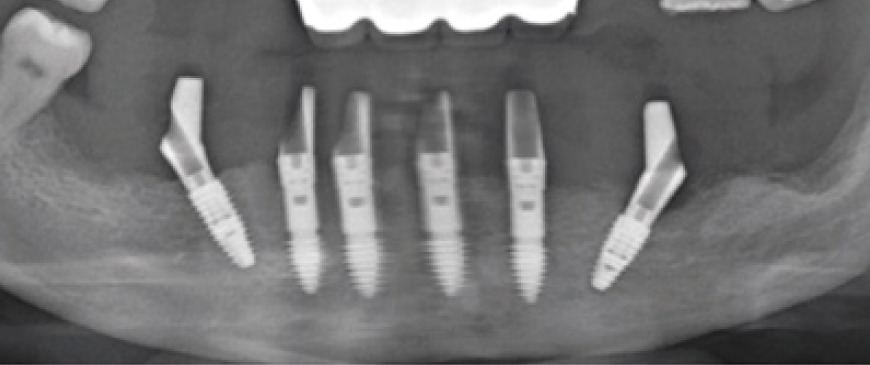
Fig 11
Panoramic image when custom abutments and PMMA bridge were placed.

Fig 12
The final prosthesis was placed approximately 3 months later, after the soft tissue stabilized.
How Have We Traditionally Managed Ridge Defects? (Thin Ridge or Socket Defect)
A Review of Conventional Approaches
Delayed Approach for Large Buccal Wall Defects
For significant buccal wall defects, a delayed approach is often used, allowing 6-8 weeks for soft tissue healing followed by GBR surgery (3-6 months of healing). This method typically requires three surgeries and extends treatment to 6 months or more.
Ignoring Small Defects
For minor defects, some clinicians skip GBR, assuming stability is sufficient. However, untreated defects may worsen over time, potentially compromising long-term implant success despite initial stability.
What if we rethought ridge defects by designing implants that minimize the need for extensive bone augmentation and reduce plaque buildup and bacterial infection in defect areas?
That's why MegaGen reimagined the solution. By combining the ARi concept for anterior atrophic thin ridges with the proven strength of BlueDiamond, which is twice as strong, and collaborating with Prof. Tomas Linkevicius' ZBLC concept, we created a new implant specifically for defective posterior regions.

Redefining Special Solution for Molar Defects:
Collaboration of BlueDiamond implant strength & ARi implant concept
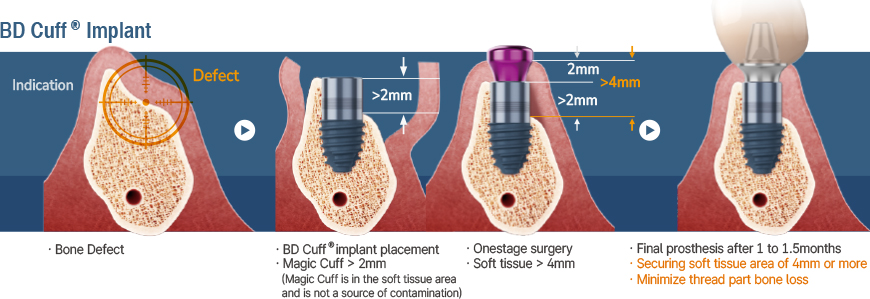
BD Cuff
- · Implant placement is possible without GBR in thin, low alveolar bone, or defective alveolar bone
- · Molar simple solution! Simple epicrestal placement
01. Minimizing bone loss
If the distance from the gingiva margin to the implant platform (rough surface) is 4mm or more, crestal bone loss is minimized
02. Higher initial stability without bone regeneration
Deep Thread & KnifeThreadⓇ Design ensure high stability even in soft bone
03. Effective prevention of peri-implantitis
Significantly lower possibility of exposure to oral bacteria due to deep placement of rough surface
04. Feel the X-FIT moment!
First with Octa, then with Keystone ensures more precise positioning & connection
05. Targeting zero fractures
100% increase in compressive strength via scientific design
06. Soft tissue friendly design
Rapid regeneration of soft tissue by facilitating generation and proliferation of HGF*-cells and subsidence prevention function (*Human Gingival Fibroblast)
07. Strong osseointegration force in basal bone maintains stability even if alveolar bone is lost
Incorporating calcium ions that create bone on S-L-A surface increases rate of osseointegration by more than 15%. Blue surface color is evidence of calcium ions!
Special Solution for Molar Defects!
Easier, Faster and More Comfortable from Complications in Lower Posterior
Almost all problems with implants start in the top 2mm. BD Cuff® eliminates the problem from the beginning.
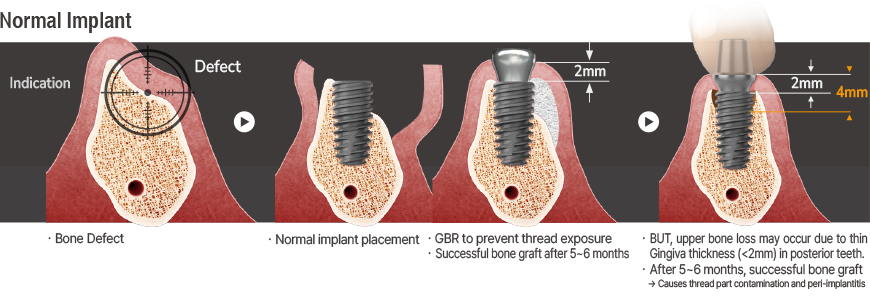
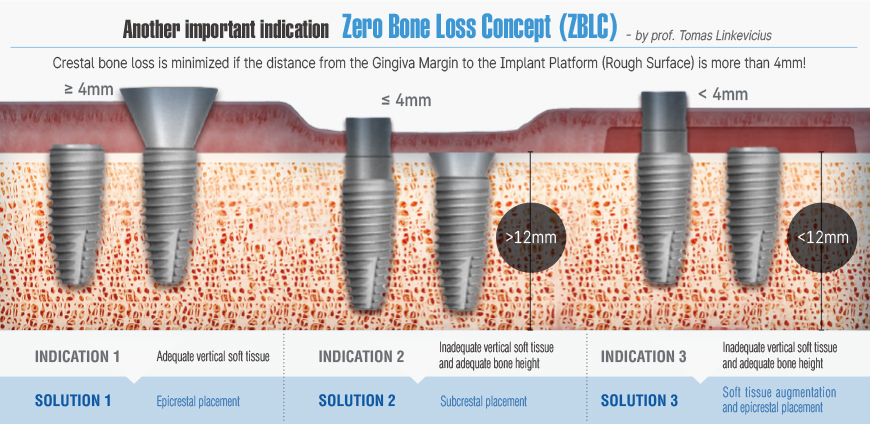
Another important indication:
Zero Bone Loss Concept (ZBLC)
by Prof. Tomas Linkevicius
The BD Cuff design, based on the Zero Bone Loss concept by Prof. Tomas Linkevicius, features a 2mm machined cuff that creates a 4mm soft tissue zone when placed in 2mm thick gingiva, preventing bone loss beyond the threaded portion. This approach ensures long-term bone stability and aligns with the Zero Bone Loss principles without requiring deep subcrestal placement.
Clinical Case
BD Cuff in Thin Ridge of the Mandibular Pontic Region

Fig 1
An elderly female patient in her mid-80s required implant treatment due to the loss of abutment teeth supporting the bridge in the right mandibular posterior region.
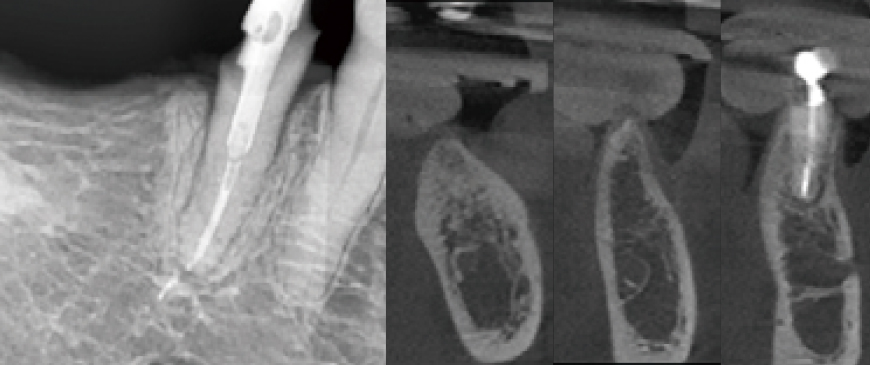
Fig 2
Intraoral and CBCT radiographic images revealed that the pontic area of the long-edentulous bridge site had developed a significantly thin ridge over time.
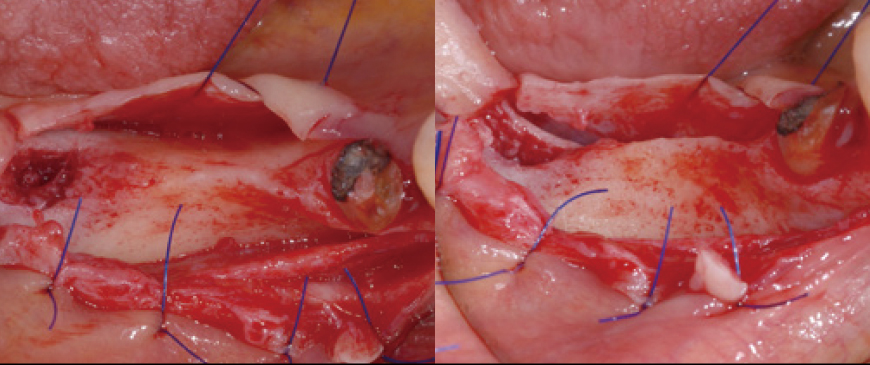
Fig 3
Upon flap elevation, it was confirmed that the first molar region also exhibited a significantly thin ridge condition.
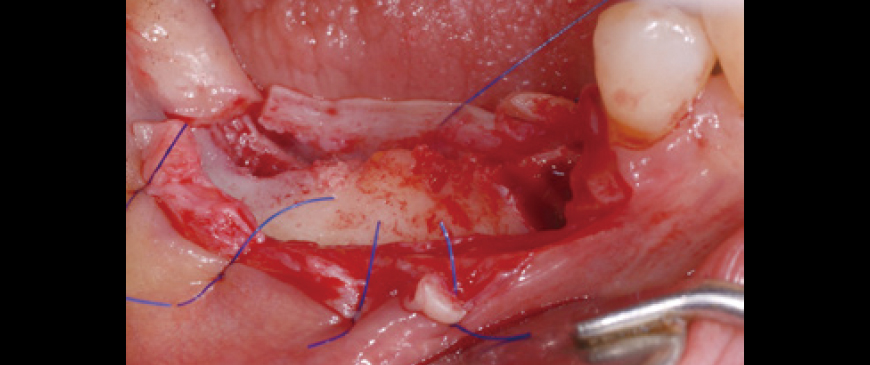
Fig 4
In cases of thin ridges, immediate drilling can be challenging due to the risk of slippage. To improve drilling accuracy and stability, a small amount of bone can be removed at the drilling point using a rongeur or similar instrument, making the drilling process significantly easier and more controlled.
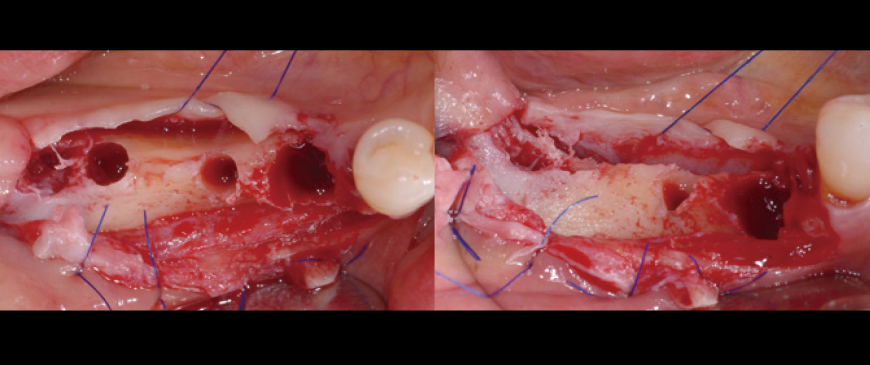
Fig 5
The osteotomy for three implants was completed, including the extraction socket of the second premolar. In the second molar region, the ridge had sufficient width, preventing dehiscence. However, in the extraction socket of the second premolar and the thin ridge area of the first molar, dehiscence occurred. Under conventional treatment protocols, active GBR (Guided Bone Regeneration) would typically be required to address these defects.
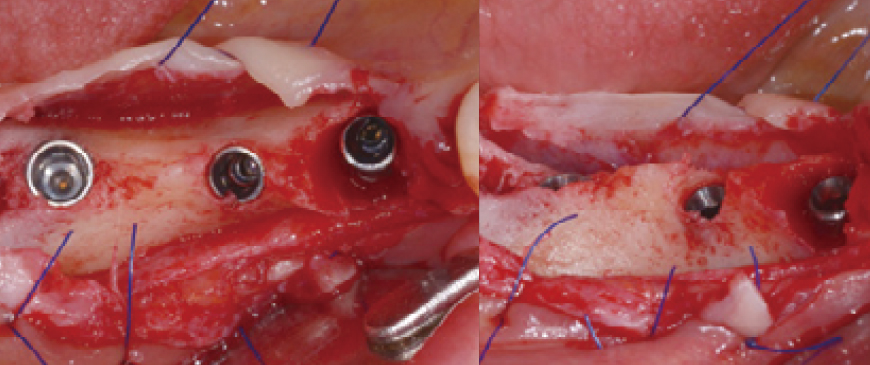
Fig 6
The three fixtures have been successfully placed. The BD Cuff implant in the second premolar extraction socket effectively covers the socket defect with its machined cuff. Additionally, the BD Cuff in the first molar region ensures that even if the thin buccal cortical bone undergoes resorption, the threads will remain covered, allowing for healthy and long-term functional stability.
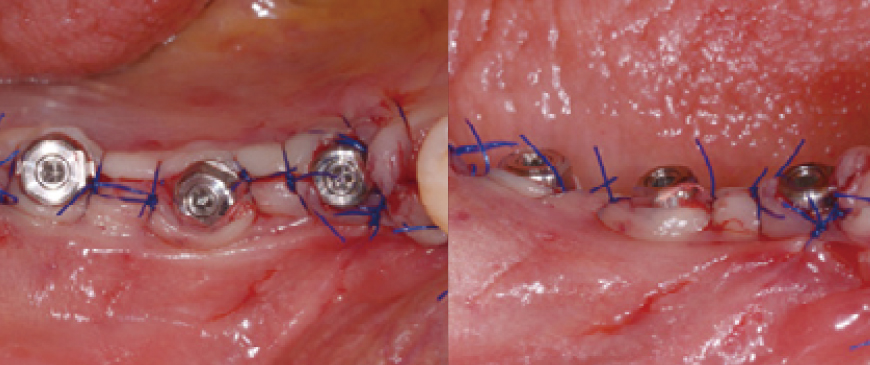
Fig 7
A small amount of allograft was placed in the second premolar extraction socket defect, while the first molar region was left untreated and simply sutured. If the patient's gingival biotype had been thin, an additional material like Ossix Volumax would have been used.
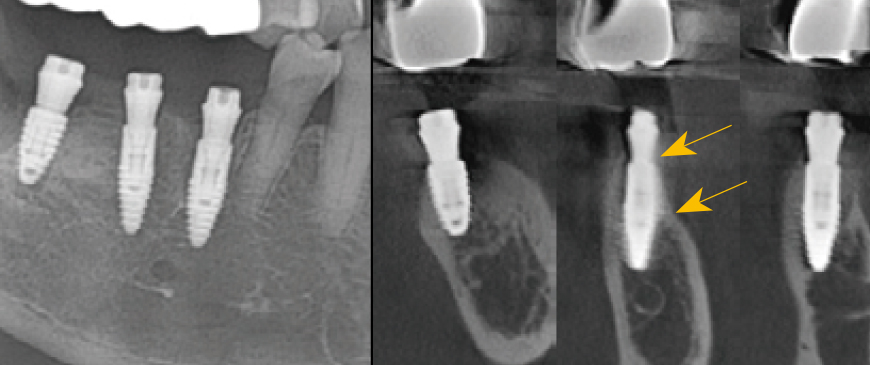
Fig 8
Postoperative panoramic and CBCT radiographs revealed minimal buccal bone thickness around the first molar implant, with the machined cuff of the BD Cuff occupying this space (indicated between the two arrows).
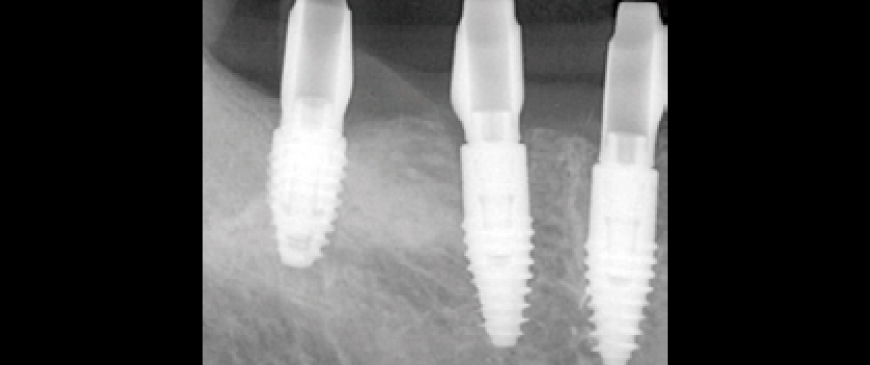
Fig 9
After approximately eight weeks, scanning was performed for impression-taking, followed by the placement of a customized abutment based on the BOPT (Biologically Oriented Preparation Technique) concept and a PMMA provisional bridge.
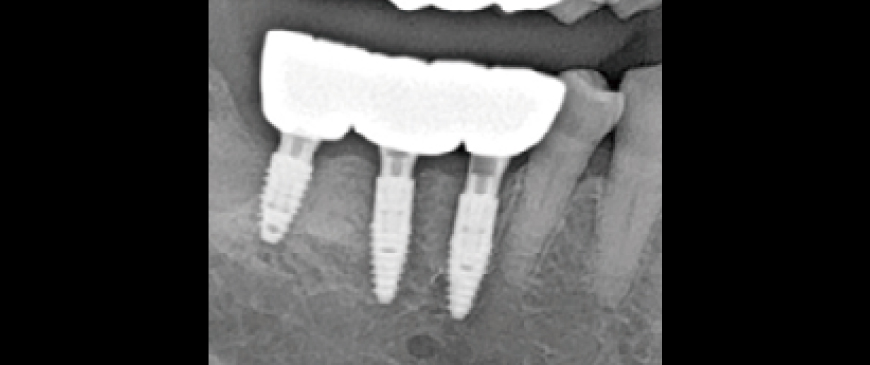
Fig 10
The provisional restoration was used for about three weeks, after which the final prosthesis was delivered.
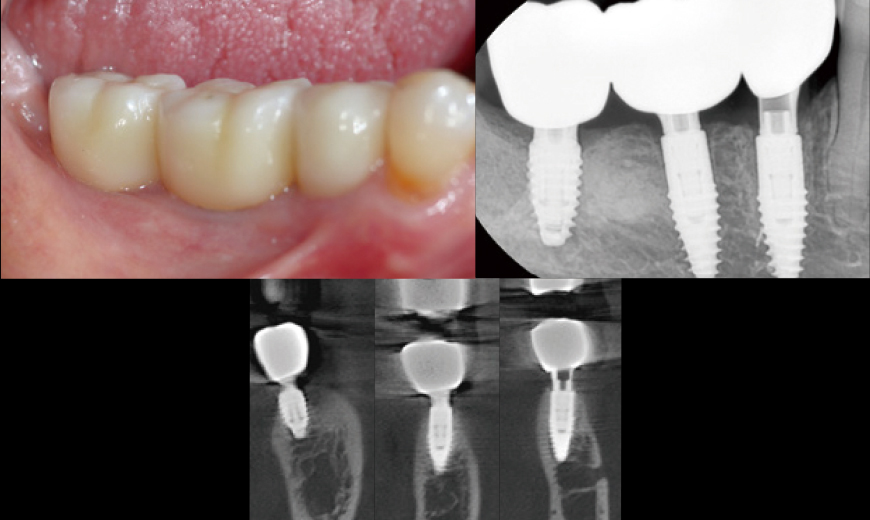
Fig 11
Intraoral Clinical Images, Radiographs, and CBCT Scans at Three Months After Loading Although this represents a relatively short follow-up period, the clinical and radiographic evaluation at three months post-loading showed comparable outcomes to conventional Blue Diamond (BD) implant cases, demonstrating no signs of compromise in stability or bone response.